Epidural Steroid Injection for Spine Care: Non-Surgical Treatment Options
Overview – Epidural Steroid Injections
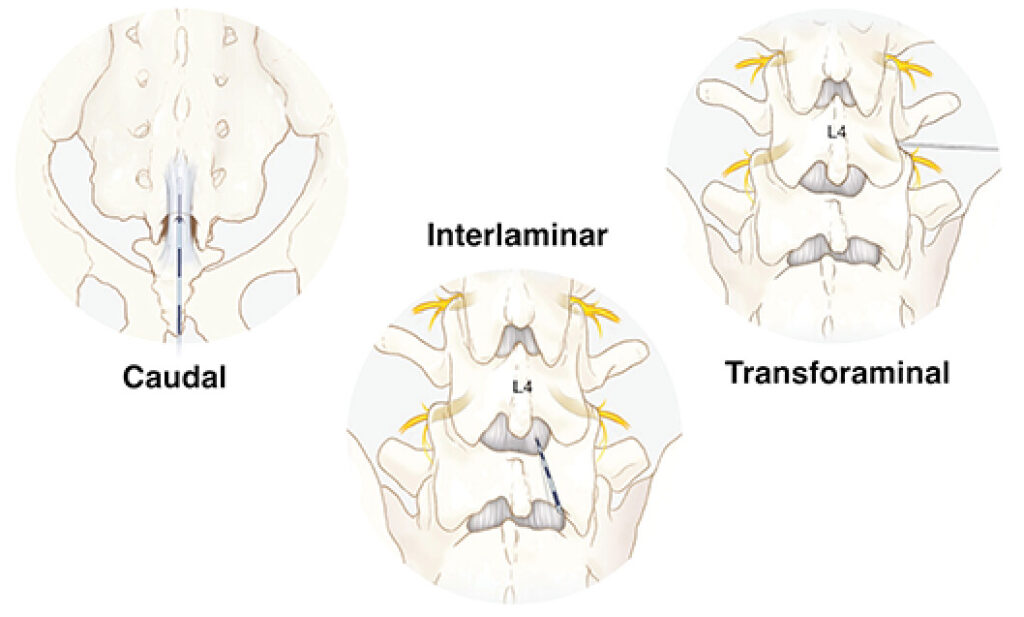
Epidural steroid injections (ESIs) are a minimally invasive, image-guided treatment designed to reduce inflammation around irritated spinal nerves. By delivering corticosteroid medication directly into the epidural space, these injections can significantly reduce radiating nerve pain such as sciatica or cervical radiculopathy.
They are most effective in conditions where nerve root inflammation is clearly identified, including:
It is important to understand that ESIs do not correct structural problems. Instead, they act as a targeted anti-inflammatory tool, often creating meaningful pain relief and improving function.
How Epidural Injections Fit Into Your Treatment Plan
Relief is often temporary, but can improve function and help guide next steps.
When Injections Don’t Work
A failed injection doesn’t mean the procedure was done incorrectly.
Common reasons include:
Pain not coming from a nerve
Structural compression that inflammation treatment can’t resolve
In these cases, the next step is usually a deeper evaluation—not repeating the same treatment.
Risks and Safety
Epidural steroid injections are generally safe when performed by experienced providers using image guidance.
Common side effects are mild and temporary, including soreness at the injection site or a short-term increase in pain. Some patients may notice brief steroid-related effects like trouble sleeping or elevated blood sugar.
Less common risks include infection, bleeding, or nerve irritation. Serious complications are rare.
The most important factor is proper patient selection. Injections work best when symptoms clearly come from an inflamed nerve and match imaging findings.
Relief typically lasts several weeks to a few months. Many patients experience around 3–6 months of benefit, but this varies based on the underlying condition and severity.
Q: How many epidural steroid injections will I need?
Most patients receive 1–3 injections depending on how they respond. If the first injection provides meaningful relief, additional injections may be considered. If it does not help, repeating it is usually reconsidered.
Q: Do epidural steroid injections fix the problem?
No. They reduce inflammation around the nerve but do not correct structural issues like a large disc herniation or spinal stenosis.
Q: When are epidural injections most effective?
They work best for radiating arm or leg pain caused by nerve irritation, especially when symptoms clearly match imaging findings.
Q: What should I do if an epidural injection doesn’t work?
If there is little or no relief, it may mean the pain is not primarily nerve-related or that the issue is more structural. This usually leads to a reassessment rather than repeating the same treatment.
Q: When should I consider a second opinion?
A second opinion is helpful if injections provide only short-term relief, symptoms continue to interfere with daily life, or the next step in treatment is unclear.
Not Sure If This Is What You’re Experiencing? Schedule an Appointment Today.