Understanding Spinal Cord Compression and When Treatment Is Needed
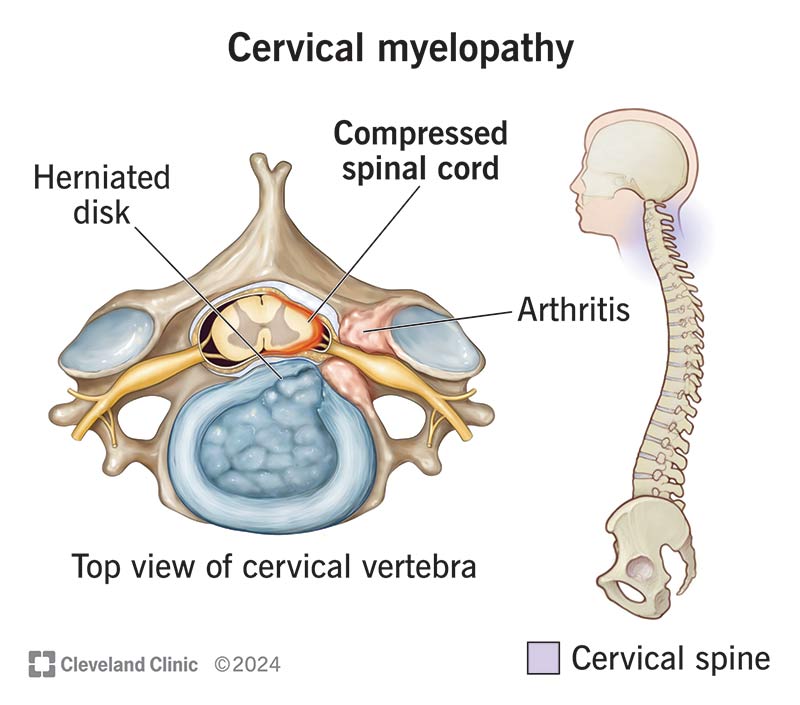
Cervical myelopathy occurs when the spinal cord in the neck becomes compressed. This can affect how signals travel between the brain and body, leading to symptoms such as hand clumsiness, balance issues, or changes in walking.
Dr. Paul focuses on early, accurate diagnosis and a thoughtful treatment approach. While spinal cord compression can sound concerning, not every case requires surgery. Many patients can be safely managed with structured non-surgical care and careful monitoring, depending on the severity and progression of symptoms.
Cervical myelopathy develops when age-related changes in the spine narrow the spinal canal and place pressure on the spinal cord. These changes may include disc degeneration, bone spurs, thickened ligaments, or disc herniation.
Unlike conditions that affect individual nerves, myelopathy involves the spinal cord itself, which is responsible for coordinating movement, balance, and fine motor control. As a result, symptoms often affect both the hands and legs rather than following a single nerve pattern.
Because this condition involves the spinal cord, recognizing symptoms early and understanding their progression is important for protecting long-term function.
Symptoms and Causes
Symptoms often develop gradually and may initially feel subtle. Over time, they can affect coordination, balance, and overall movement.
The most common cause is age-related degeneration of the cervical spine. As discs lose height and joints develop arthritis, the space available for the spinal cord can gradually narrow. In some cases, a naturally smaller spinal canal can increase the likelihood of developing symptoms.
How is Cervical Myelopathy Diagnosed?
Diagnosis begins with a detailed clinical evaluation focused on neurological function. This includes assessing coordination, balance, reflexes, and hand dexterity to determine whether the spinal cord is affected.
MRI is the most important imaging tool, as it allows direct visualization of spinal cord compression and any associated changes within the cord itself. X-rays may be used to evaluate alignment and structural changes, while additional testing can help differentiate myelopathy from other conditions such as peripheral nerve disorders.
A precise diagnosis is essential, as treatment decisions are based not only on imaging but also on how symptoms are progressing over time.
For patients with mild or stable symptoms, non-surgical management can be a safe and effective approach. The focus is on maintaining function, reducing strain on the spine, and closely monitoring for any signs of progression.
Physical therapy may help improve posture, strengthen supporting muscles, and enhance balance and coordination. Medications can be used to manage discomfort or nerve-related symptoms when needed. Activity modifications, such as avoiding high-impact movements or excessive neck strain, also play an important role in protecting the spinal cord.
Regular follow-up is essential. Monitoring ensures that any changes in strength, coordination, or walking are identified early so treatment can be adjusted if necessary.
Surgery is considered when there is clear evidence that the spinal cord is under increasing stress or when neurological function begins to decline. This may include worsening hand coordination, increasing difficulty with walking or balance, or imaging findings that show significant cord compression.
In these situations, surgery is recommended to relieve pressure on the spinal cord and prevent further neurological decline. The decision is made carefully, based on both clinical findings and the patient’s overall condition.
The goal is always to protect long-term function. Treatment is approached as a continuum, with surgery considered only when it provides a clear benefit over continued observation.
Cervical myelopathy happens when the spinal cord in the neck is compressed, usually from arthritis, disc changes, or thickened ligaments. Because the spinal cord controls both arms and legs, symptoms often involve balance, coordination, hand function, and walking rather than neck pain alone.
Q: What are the earliest symptoms of cervical myelopathy?
Early symptoms can be subtle and easy to overlook. Many patients notice hand clumsiness, dropping objects, slower handwriting, trouble with buttons or zippers, or a mild sense of imbalance before they ever develop significant neck pain.
Q: How do I know if cervical myelopathy is getting worse?
Worsening hand dexterity, more frequent falls, increasing leg stiffness, new weakness, or bladder and bowel changes can all suggest progression. Changes over time are especially important, which is why repeat exams are often as valuable as the MRI itself.
Q: Is cervical myelopathy always an emergency?
Not always. Some mild cases can be monitored closely and treated conservatively at first. However, progressive neurologic decline or clear spinal cord dysfunction should be evaluated promptly so treatment is not delayed when the cord is at risk.
Q: Can physical therapy fix cervical myelopathy?
Physical therapy can improve posture, gait mechanics, balance, and conditioning, but it does not remove spinal cord compression. It is best viewed as supportive care, not a substitute for surgery when neurologic decline is clearly developing.
Q: What is the best test for cervical myelopathy?
MRI is usually the most helpful test because it shows the spinal cord, the amount of canal narrowing, disc herniations, and whether there are signal changes inside the cord. Imaging still needs to be matched to symptoms and exam findings.
Q: Can cervical myelopathy stay stable for years?
Yes, some patients remain stable for long periods, especially if symptoms are mild and there is no clear progression on neurologic exam. Others worsen more quickly, which is why regular follow-up and attention to functional changes matter.
Q: What happens if cervical myelopathy is left untreated?
If a progressive case is ignored, spinal cord compression can lead to permanent loss of balance, hand coordination, strength, and walking function. The goal of timely treatment is not just pain relief, but protecting the spinal cord from lasting injury.
Noticing Changes in Coordination or Balance? Schedule an Appointment Today.
1. Donnally CJ III et al. Cervical Myelopathy. StatPearls [Internet]. NCBI Bookshelf; updated 2023. 2. McCormick JR et al. Cervical Spondylotic Myelopathy: A Guide to Diagnosis and Management. J Am Acad Orthop Surg. 2020. 3. Fehlings MG et al. A Clinical Practice Guideline for the Management of Patients With Degenerative Cervical Myelopathy. Global Spine J. 2017.
4. Pahuta M et al. Nonoperative Care Versus Surgery for Degenerative Cervical Myelopathy: Updated Evidence. Global Spine J. 2024. 5. Kane SF et al. Degenerative Cervical Myelopathy: Recognition and Management. Am Fam Physician. 2020. 6. North American Spine Society (NASS). Cervical Stenosis & Myelopathy – Patient and Clinical Resources. 2023. 7. National Spine Health Foundation. Cervical Myelopathy Explained. 2023.