Non-Surgical Solutions for Low Back Pain, Instability, and Nerve Compression
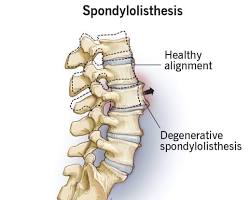
Lumbar spondylolisthesis occurs when one vertebra in the lower spine shifts forward relative to the one beneath it. This forward slippage can create instability in the spine and may contribute to nerve compression, leading to both lower back pain and symptoms in the legs.
Dr. Paul focuses on accurate diagnosis and structured non-surgical care to improve stability, reduce symptoms, and restore function. In most cases, this condition can be effectively managed without surgery through targeted therapy and long-term movement strategies.
Lumbar spondylolisthesis, often referred to as a “slipped vertebra,” most commonly occurs at the L4–L5 and L5–S1 levels of the spine.
It frequently develops as a result of degenerative changes, including disc wear and facet joint arthritis, which reduce the stability of a spinal segment. As the vertebra shifts forward, it can narrow the spinal canal and place pressure on the nerves that travel into the legs.
This condition often overlaps with lumbar spinal stenosis, which explains why many patients experience symptoms that worsen with standing or walking and improve when sitting or leaning forward.
Symptoms and Causes
Symptoms vary depending on the degree of slippage and nerve involvement.
Diagnosis begins with a thorough clinical evaluation focused on understanding how symptoms change with movement and activity. Physical examination assesses posture, gait, strength, and neurological function, helping determine whether nerve involvement is present.
Standing X-rays are essential for identifying vertebral slippage and assessing stability, particularly when comparing movement between positions. MRI provides detailed information about nerve compression, spinal canal narrowing, and associated degenerative changes, while CT scans may be used when evaluating bony structures in greater detail.
This comprehensive approach ensures that both structural findings and clinical symptoms are properly aligned.
Most patients with lumbar spondylolisthesis, particularly those with low-grade slippage, can achieve meaningful improvement without surgery.
Treatment focuses on improving spinal stability and reducing stress on affected segments. Physical therapy plays a central role, emphasizing core strengthening, flexibility, and movement patterns that support the spine. Medications may be used to manage inflammation and nerve-related symptoms, while injections can provide relief for persistent irritation.
Long-term success is strongly influenced by consistent movement, proper mechanics, and maintaining strength in the muscles that support the spine.
When Is Surgery Necessary?
Surgery is considered only when symptoms progress or do not improve with comprehensive non-surgical care.
This may include:
Persistent or worsening leg pain despite treatment
Progressive weakness or neurological symptoms
Significant limitations in walking or standing
Evidence of instability or worsening vertebral slippage
Rare cases involving bowel or bladder dysfunction (urgent evaluation required)
When needed, treatment is carefully tailored to relieve nerve compression and restore spinal stability while minimizing disruption to surrounding structures.
Lumbar Spondylolisthesis:
Frequently asked Questions (FAQs)
Q: What is lumbar spondylolisthesis?
Lumbar spondylolisthesis is a condition in which one vertebra slips forward relative to the vertebra below it. It may be caused by degeneration, a pars defect or stress fracture, or less commonly by trauma or prior surgery.
Q: What symptoms does lumbar spondylolisthesis cause?
Symptoms may include low back pain, stiffness, leg pain, numbness, or a sense of heaviness in the legs. Some patients mainly notice trouble standing or walking for long periods rather than sharp back pain.
Q: What is neurogenic claudication and how is it related to spondylolisthesis?
Neurogenic claudication is leg pain, heaviness, weakness, or tingling that gets worse with standing or walking and improves with sitting or bending forward. It commonly occurs when degenerative spondylolisthesis contributes to lumbar spinal stenosis.
Q: How is lumbar spondylolisthesis diagnosed?
Diagnosis usually starts with standing X-rays, often including flexion-extension views, to show the amount of slippage and whether instability is present. MRI is useful when leg symptoms suggest nerve compression or spinal stenosis.
Q: Can lumbar spondylolisthesis be treated without surgery?
Yes. Many people improve with physical therapy, core stabilization, posture and lifting changes, weight management, walking programs, and selective injections. Surgery is not automatically necessary just because slippage is seen on imaging.
Q: What role does a pars fracture play in spondylolisthesis?
A pars fracture, also called an isthmic defect, can allow one vertebra to slip forward over another. This is a different mechanism from degenerative spondylolisthesis, which is usually driven by arthritis and disc wear.
Q: When should surgery be considered?
Surgery is usually considered when there is progressive weakness, disabling neurogenic claudication, persistent pain despite a strong non-surgical program, or documented instability that clearly matches the symptoms.
Q: What is the long-term outlook for lumbar spondylolisthesis?
Many patients do well for years with conservative care, especially when the slippage is low grade and stable. The key is matching treatment to symptoms, not reacting to the imaging alone.
Not Sure If This Is What You’re Experiencing? Schedule an Appointment Today.
1. Kalichman L et al. Spondylolisthesis: Prevalence, Risk Factors, and Clinical Features. StatPearls, NCBI Bookshelf; 2024. 2. Weinstein JN et al. Surgical vs Nonoperative Treatment for Degenerative Spondylolisthesis: SPORT Trial. N Engl J Med. 2007. 3. Försth P et al. Decompression with or without Fusion in Degenerative Lumbar Spondylolisthesis. N Engl J Med. 2016. 4. Kreiner DS et al. NASS Clinical Guidelines for Degenerative Lumbar Spondylolisthesis. 2022. 5. National Spine Health Foundation. Educational Resources on Spondylolisthesis. 2024.