Understanding What the Science, Data, and Research Shows About Lateral Interbody Fusion (XLIF)
Understanding When This Approach Is Used And How It Supports Stability
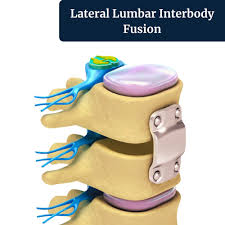
Lateral interbody fusion, often referred to as XLIF or transpsoas lumbar interbody fusion, is a minimally invasive procedure used to treat specific types of spinal instability, disc collapse, and nerve compression.
Dr. Paul uses this approach selectively when it matches the patient’s anatomy and underlying condition. By accessing the spine from the side, the procedure allows for restoration of disc height and alignment while minimizing disruption to surrounding muscles and soft tissues.
When Is Lateral Interbody Fusion Most Appropriate?
Lateral interbody fusion is most effective when there is a clearly defined structural issue that can be improved by restoring disc height and stabilizing the spine. This includes conditions such as low-grade degenerative spondylolisthesis, segmental instability, and disc space collapse that leads to narrowing around the nerves.
The best outcomes are typically seen when symptoms persist despite appropriate non-surgical care and when imaging findings clearly match the patient’s clinical presentation. In these cases, restoring the height of the disc space can relieve pressure on the nerves indirectly while also improving overall alignment.
Patient anatomy also plays an important role. Not every patient is a candidate for a lateral approach, and careful evaluation is required to determine whether this technique is appropriate.
How Does Lateral Interbody Fusion Relieve Nerve Compression?
Unlike traditional posterior approaches, lateral interbody fusion works by restoring the height of the disc space rather than directly removing tissue around the nerves. By expanding the space between vertebrae, the openings where nerves exit the spine are widened.
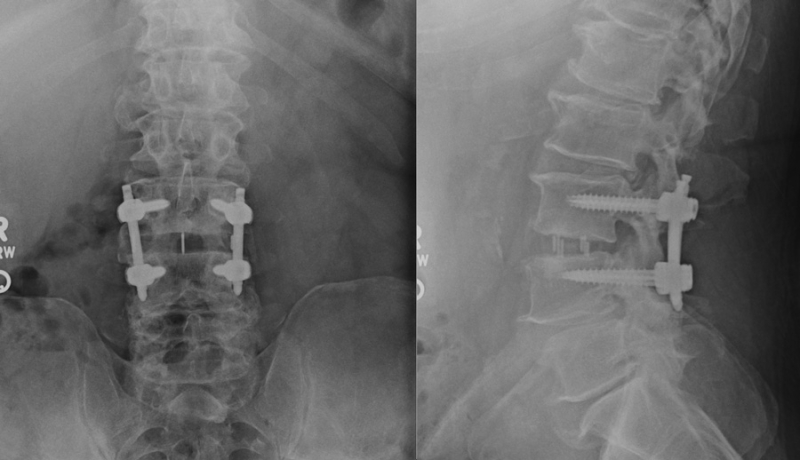
At the same time, the placement of an interbody implant stabilizes the spinal segment. This combination of restoring height and stabilizing motion allows the procedure to address both nerve compression and underlying instability in a single approach.
What Outcomes Are Reported In The Research?
The published literature on lateral interbody fusion shows consistent improvement in pain, function, and radiographic alignment when the procedure is used for the right indications.
Patients commonly experience meaningful improvements in disability scores, back pain, and leg pain. The technique is particularly effective at restoring disc height and foraminal dimensions, which contributes to relief of nerve-related symptoms.
A recent meta-analysis focused on XLIF reported good clinical and radiographic outcomes with a low rate of serious complications. While exact improvement rates vary depending on the study and patient population, the majority of appropriately selected patients experience substantial benefit.
Understanding Risks And Approach-Specific Factors
Lateral interbody fusion has a favorable safety profile, but its risks differ from traditional posterior approaches because the procedure passes through the psoas region near the lumbar plexus.
The most commonly reported serious complications include nerve-related injury, which occurs in a small percentage of cases. Other rare complications include gastrointestinal issues or vertebral fracture.
More commonly, patients may experience temporary symptoms such as thigh numbness, hip flexor weakness, or psoas irritation early after surgery. These symptoms are usually transient and improve over time.
Overall complication rates reported in the literature include both minor and temporary issues. When focusing on long-term outcomes, serious complications remain relatively uncommon, particularly when the procedure is performed with careful technique and neuromonitoring.
Want To Better Understand Your Surgical Options? Schedule your appointment today.
Lateral interbody fusion is best understood as one of several surgical options rather than a universal solution. Compared to posterior fusion techniques, it often results in less muscle disruption, reduced blood loss, and a faster early recovery.
At the same time, the lateral approach introduces unique considerations related to the lumbar plexus, which is why patient selection is critical. For some patients, a posterior or anterior approach may be more appropriate depending on their anatomy and condition.
The research consistently supports a central principle. This procedure works best when symptoms are clearly tied to structural problems such as instability, disc collapse, or foraminal narrowing that can be improved by restoring height and stabilizing the spine.
For appropriately selected patients, most improve, many improve substantially, and a smaller group may require additional treatment over time.
References
Lang G, Perrech M, et al. Radiographic and clinical outcomes of lateral lumbar interbody fusion: a systematic review and meta-analysis of 1,080 patients. Spine. 2014;39(24):E1442-E1451.
Wang TY, Nayar G, et al. Indirect decompression and foraminal height restoration with lateral lumbar interbody fusion (LLIF): a radiographic and clinical analysis. World Neurosurgery. 2017;106:911-920.
Elowitz EH, Yanni DS, et al. Evaluation of indirect decompression of the lumbar spinal canal following minimally invasive lateral interbody fusion, using magnetic resonance imaging. Journal of Neurosurgery: Spine. 2016;24(6):880-885.
Li HM, Zhang RJ, Shen CL. Radiographic and clinical outcomes of lateral lumbar interbody fusion versus transforaminal lumbar interbody fusion in the treatment of degenerative lumbar diseases: a meta-analysis. Journal of Orthopaedic Surgery and Research. 2020;15(1):105.
Zhang H, Zhou C, et al. Lateral lumbar interbody fusion (LLIF) vs. transforaminal lumbar interbody fusion (TLIF) in degenerative lumbar disease: a systematic review and meta-analysis. Frontiers in Surgery. 2021;8:765507.
Rodgers WB, Gerber EJ, Patterson J. Intraoperative and early postoperative complications in extreme lateral interbody fusion: an analysis of 600 cases. Spine. 2011;36(1):26-32.
Ahmadian A, Deukmedjian AR, et al. The use of lateral transpsoas approach for lumbar interbody fusion: clinical outcomes, complications, and radiographical results in 100 consecutive cases. Journal of Spinal Disorders & Techniques. 2015;28(3):113-119.
Oliveira L, Marchi L, et al. Radiographic and clinical results after less invasive approach for treatment of degenerative lumbar spine disease. The Spine Journal. 2010;10(9):S49.