Relief for Neck Pain, Nerve Compression, and Radiating Arm Symptoms
A cervical herniated disc occurs when one of the discs in the neck develops a small tear, allowing its inner material to push outward and irritate nearby nerves. This can lead to neck pain, radiating arm pain, numbness, or weakness that affects everyday activities.
A cervical herniated disc occurs when one of the discs in the neck develops a small tear, allowing its inner material to push outward and irritate nearby nerves. This can lead to neck pain, radiating arm pain, numbness, or weakness that affects everyday activities.
Dr. Paul takes a diagnosis-first approach, focusing on identifying the exact source of symptoms before recommending treatment. While the condition may sound serious, most cervical disc herniations improve over time with structured non-surgical care that reduces inflammation and restores normal movement.
The cervical spine is made up of vertebrae separated by discs that absorb stress and allow the neck to move smoothly. Over time, or with repeated strain, the outer layer of a disc can weaken or develop a small tear. When this happens, the inner gel-like material can shift outward.
If that material presses on a nearby nerve, it can cause symptoms along the nerve’s pathway. This is known as cervical radiculopathy and is one of the most common causes of arm pain in adults.
The levels C5–C6 and C6–C7 are most often affected, which is why symptoms frequently travel into the shoulder, arm, or hand.
Symptoms and Causes
Symptoms depend on the location and severity of the herniation but often include:
Increased pain with coughing, sneezing, or neck movement
In many cases, herniated discs develop gradually due to age-related changes. They can also occur from repetitive strain, poor posture, or sudden movement. Even when symptoms are present, they often improve as inflammation settles and the body adapts.
How is a Cervical Herniated Disc Diagnosed?
I have processed this batch of code, incorporating the internal links to your directory. Per your new instructions, all linked text is now bold in addition to being styled in blue.
Diagnosis starts with a detailed clinical evaluation, focusing on how symptoms behave and whether a specific nerve is involved. A physical exam helps assess strength, reflexes, and sensation to better understand the source of the problem.
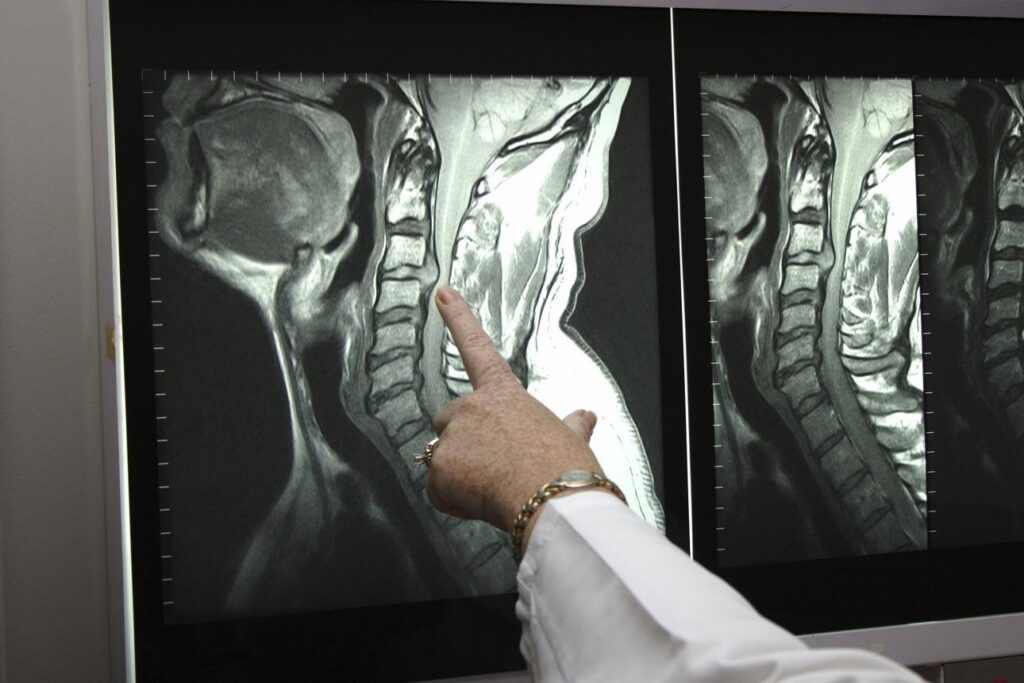
MRI is the most useful imaging tool for confirming a disc herniation and identifying nerve compression. X-rays may be used to evaluate alignment, while additional testing can help clarify more complex cases.
The goal is to match imaging findings with symptoms—ensuring that treatment is based on what is actually causing discomfort, not just what appears on a scan.
Care is designed to reduce pressure on the nerve while supporting long-term recovery and prevention.
When Is Surgery Necessary?
Surgeryis typically considered only when symptoms do not improve with non-surgical care or when neurological issues begin to develop. This may include progressive weakness, persistent pain, or imaging findings that clearly match the symptoms being experienced.
When needed, treatment focuses on relieving pressure on the affected nerve while preserving as much natural movement as possible.
A cervical herniated disc occurs when disc material in the neck pushes outward far enough to irritate or compress a nearby nerve root. This can cause neck pain, shoulder pain, arm pain, tingling, numbness, or weakness.
Q: Is a cervical herniated disc the same as a slipped disc?
Yes. Terms like slipped disc, ruptured disc, disc protrusion, disc extrusion, and herniated disc are often used to describe similar problems. The exact word on the MRI matters less than whether the finding matches your symptoms.
Q: What are the most common symptoms of a cervical disc herniation?
Many patients notice radiating arm pain, tingling in the fingers, numbness, or weakness in the arm or hand. Neck pain may be present, but some people are bothered far more by the arm symptoms than by the neck itself.
Q: Can a cervical herniated disc heal on its own?
Yes. Most cervical disc herniations improve with time and conservative care. The body often reduces inflammation and may even reabsorb part of the herniated material over time.
Q: How long does recovery usually take?
Many patients improve substantially over 6 to 12 weeks, although the timeline varies depending on the size of the herniation, the amount of nerve irritation, and how the person responds to physical therapy and medication.
Q: What treatments help most before surgery is considered?
The most helpful first steps are usually posture correction, guided physical therapy, anti-inflammatory medication, staying active within reason, and occasionally a carefully selected injection when nerve pain remains severe.
Q: When is surgery considered for a cervical herniated disc?
Surgery is considered when symptoms stay disabling despite a thorough non-surgical program or when there is progressive weakness, significant loss of function, or spinal cord compression that makes waiting unsafe.
Q: Can I still exercise with a cervical herniated disc?
Usually yes, but it should be smart, controlled, and symptom-guided. Gentle movement, walking, and therapeutic exercise are often helpful, while aggressive neck loading or high-impact activity may need to be avoided temporarily.
Not Sure If This Is What You’re Experiencing? Schedule an Appointment Today.
1. Bono CM, Ghiselli G, et al. An Evidence-Based Clinical Guideline for the Diagnosis and Treatment of Cervical Radiculopathy from Degenerative Disorders. Spine J. 2011. 2. Eubanks JD. Cervical Radiculopathy. StatPearls [Internet]. NCBI Bookshelf; updated 2024. 3. Brinjikji W et al. MRI Findings in Asymptomatic Populations. AJNR Am J Neuroradiol. 2015. 4. Wainner RS, et al. Diagnostic Accuracy of Clinical Tests for Cervical Radiculopathy. Spine. 2003. 5. North American Spine Society (NASS). Clinical Guidelines for Cervical Radiculopathy. 2023. 6. National Spine Health Foundation. Patient Education on Cervical Spine Disorders. 2024.